[Guide] What Every CRT Business Needs to Know in 2026 to Reduce Denials and Protect Revenue
Table of Contents
The Reality of CRT in 2026
The CRT industry is not getting simpler.
Reimbursement rules are evolving, documentation expectations are becoming more precise, and payers are enforcing policies more consistently than ever before.
What has changed is not just the rules themselves, but also how tightly they are being applied.
The small gaps that teams used to work around are now showing up as:
- Denied claims
- Delayed payments
- Increased audit risk
- Revenue that never gets captured
This is not a knowledge problem. Most teams understand the basics. It is an execution problem.
To help clarify where things are breaking down, we partnered with
Dan Fedor, Director of Reimbursement and Education at
U.S. Rehab, to walk through the most common issues CRT providers are facing today.
Where Things Actually Go Wrong
Across the webinar and follow-up discussion, five core areas consistently surfaced:
- Denials driven by misapplied policy
- Revenue leakage from missed billing opportunities
- Documentation and compliance gaps, especially around LMNs
- Misunderstanding of telehealth rules
- Confusion around replacement and repair requirements
These are not isolated issues.
They are all tied to how workflows are structured and how consistently teams follow them.
The Top 5 CRT Denials
Denials are rarely unpredictable. They tend to follow the same patterns over and over again.
What makes them difficult is that they are often caused by small technical missteps, not major oversights.
1. Rent vs. Purchase Guidelines Not Met
This is one of the most common denial drivers because it requires both technical understanding and proper documentation.
At a policy level:
- ALL power wheelchair bases (K0813-K0864) are in the
capped rental category
- Complex rehab power wheelchair bases (K0835-K0864) have a first month purchase option as well as ALL accessories used on those bases
Where this breaks down in practice is documentation.
A required step is the purchase option letter. It must be given to the beneficiary, signed and dated, and clearly reflect the selection of rental or purchase. If this is missing or incomplete, the claim will not hold.
The issue is not that teams do not know this rule. It is that workflows do not consistently enforce it.
2. Billing and Fee Schedule Misalignment
This is where many teams lose control of claims without realizing it.
The rules are highly specific:
- K0813 through K0831 must be billed as a 13-month rental
- Capped rental items only show RR on the fee schedule
Calculations matter:
- For power wheelchair bases with a purchase option (K0835-K0864), the purchase allowable is the RR divided by .15
- For power wheelchairs without a purchase option (K0813-K0831), the total amount after 13 months of rental is the RR divided by .15 x 1.05
- For capped rental accessories with a purchase option (used on K0835- K0864), the purchase allowable is the RR x 10
- For capped rental items without a purchase option, the total amount after 13 months rental is RR x 10.5
Inexpensive or routinely purchased items, or IRP items, have a first-month purchase option regardless of the base code they are used on.
Examples include:
- E2363 (batteries)
- E2603 (skin protection cushion)
- E0973 (detachable height adjustable arms)
These items can be purchased on all power bases K0813-K0864.
Manual wheelchairs introduce another layer of complexity. All manual wheelchairs are in the capped rental category and can only be rented for 13 months, except for the K0005 ultra lightweight wheelchair, which is in the IRP category and can be purchased in the first month.
However, capped rental accessories can only be rented when used on all manual chairs, including the K0005, even though the K0005 itself is a purchase base.
IRP items show NU, UE, and RR on the fee schedule, and each reflects the allowable based on how the item is provided:
- NU = new product
- UE = used product, with an allowable of 75 percent of new
- RR = rent
- al, or NU divided into 10 equal payments
Bilateral items can be billed in one of two ways:
- One line with 2 units and no RT/LT
- Separate lines with 1 unit per line, which requires RT/LT
A quick way to validate classification is by looking at the fee schedule:
- IRP items show NU, UE, and RR
- Capped rental items only show RR
Even experienced teams get tripped up here, not because the rules are unclear, but because they are applied inconsistently across orders.
3. Incorrect Date Sequencing
This is one of the most technical areas and one of the most common sources of denials.
The required sequence is strict:
- Face to face evaluation
- LMCP wheelchair evaluation
- ATP assessment
- SWO or DSWO
The nuance that often gets missed is what “complete” actually means.
Completion means the encounter is:
- Performed
- Signed
- Dated
- Co-signed when applicable
Only after that can the SWO be dated.
SWO and DSWO cannot be dated prior to completion of the face-to-face and the LMCP wheelchair evaluation.
The ATP assessment cannot be completed prior to the LMCP wheelchair evaluation, although it can occur on the same day.
Additional requirements include:
- The SWO must be 100 percent handwritten by the ordering practitioner or 100 percent electronic health record for PMDs
- The SWO must be written within 6 months of the face-to-face
- The PMD must be delivered within 6 months of the date on the prior auth affirmation letter
Another important clarification is that there is no “start date” on the SWO. Only the signature date matters, and it must follow the completed evaluations.
This is a perfect example of where teams feel compliant but are technically out of alignment.
4. Beneficiary Does Not Meet Coverage Criteria
This is where clinical understanding and policy definitions must match exactly.
Group 3 power wheelchairs require a qualifying condition, including neurological conditions, myopathies, or congenital skeletal deformities, and that condition must be the primary cause of the mobility limitation.
Examples include:
- Amyotrophic Lateral Sclerosis (ALS)
- Spinal cord injuries resulting in quadriplegia
- Stroke (CVA) with hemiplegia
- Late-stage Parkinson's
- Late-stage Multiple Sclerosis (MS)
- Cerebral Palsy
- Muscular Dystrophy
A common misunderstanding is assuming that symptoms qualify.
For example, a Group 3 power wheelchair would not be appropriate for a beneficiary with diabetes and peripheral neuropathy. Although peripheral neuropathy affects the nerves, it does not meet the definition of a qualifying neurological condition. It is a symptom of another disease.
The Power Mobility Device Local Coverage Determination (LCD) specifically states that the patient must have a qualifying condition that meets coverage criteria. That is why a beneficiary with peripheral neuropathy does not qualify for a Group 3 power wheelchair on that basis alone.
The emphasis here is important. Coverage is not based on how severe a condition feels. It is based on how it is defined in policy.
5. Incorrect Place of Service
This is one of the most straightforward rules, yet it still causes frequent denials.
Medicare Part B only covers Durable Medical Equipment (DME) when the beneficiary resides in what is considered “home.”
Here is a quick look at DME coverage status based on Place of Service (POS) codes:
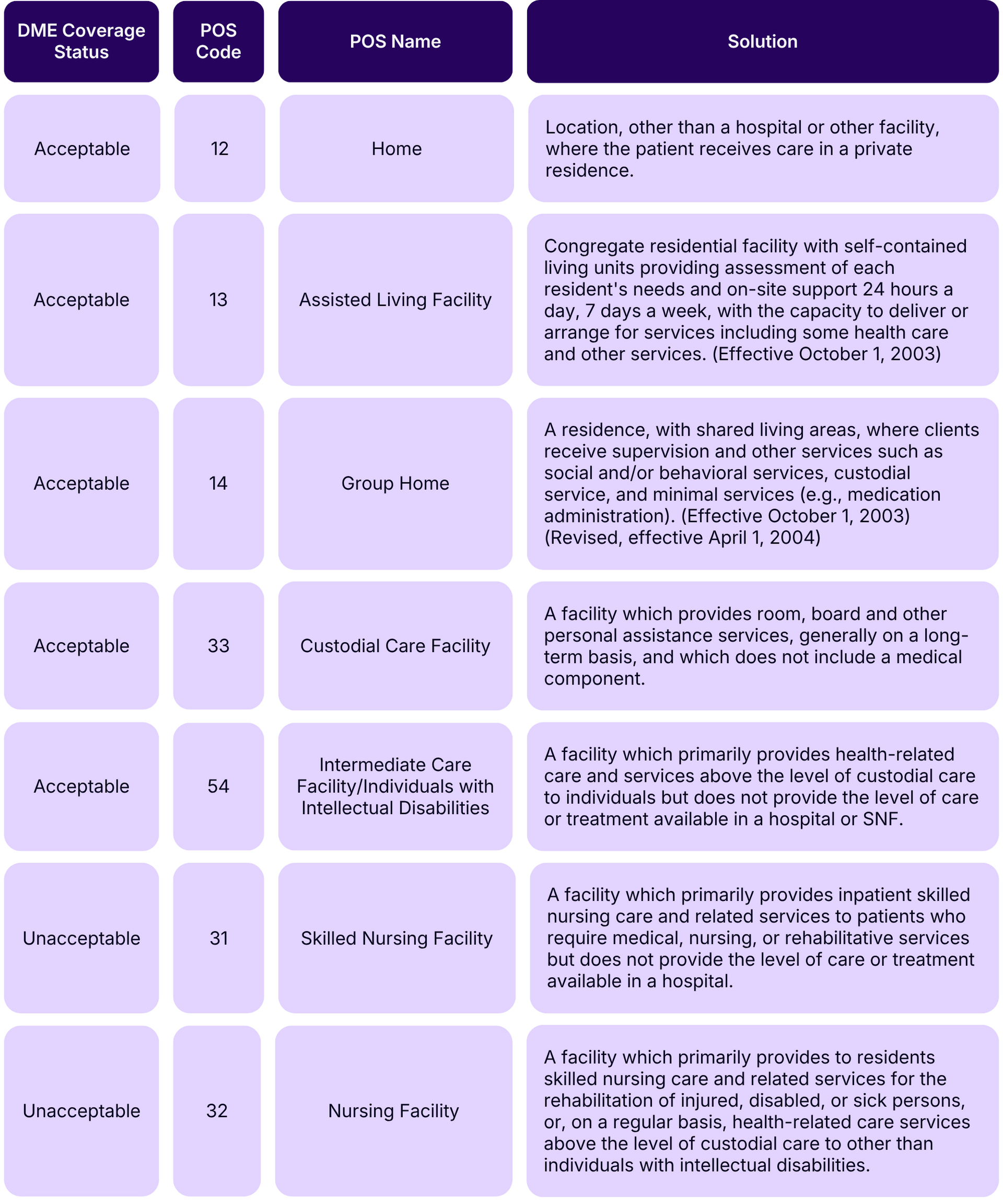
Proper use of POS 31 and 32 is especially important:
- POS 31 (Skilled Nursing Facility)
- When the beneficiary is under a Part A Medicare stay, up to 100 days, the result is a Contractual Obligation (CO) denial and the item is not separately payable.
- POS 32 (Nursing Facility)
- When the beneficiary is outside a Part A Medicare stay, after 100 days or on private pay, the result is a Patient Responsibility (PR) denial and the item is not covered.
Even if everything else is correct, the wrong POS code will result in denial.
This is a simple rule, but it requires consistent attention at intake and billing.
The Hidden Cost of Revenue Leakage
Denials are visible. Revenue leakage is not.
A significant portion of lost revenue comes from services that were never billed or were not billed correctly,
The most common gaps include:
- Not using the KU modifier on accessories and repair parts used on K5, E1161, and Group 3 power bases
- Not billing labor (K0739) when parts are under warranty
- Not maximizing labor reimbursement with itemized labor time in minutes per part
- Not billing for temporary replacement equipment (K0462) when provided
- Not submitting unassigned claims when necessary, such as battery replacements
- Not correctly documenting abuse or neglect, then charging the beneficiary when appropriate with an ABN
- Not charging the beneficiary for routine maintenance
- Not billing Medicare for extensive maintenance as labor (K0739)
Where This Gets Misunderstood
If a manufacturer covers the part but not the labor, the labor can still be billed to Medicare.
Even something as simple as removing and reinstalling equipment can qualify as billable labor, depending on the situation.
Another common issue is documentation. Medicare may deny labor if the time and HCPCS breakdown are not detailed enough. In many cases, appeals are successful when more detail is provided.
The takeaway is that billing is not just about submitting a claim. It is about clearly telling the story of what was done and why.
AI in CRT and LMN Generator Compliance
AI is becoming more common in documentation workflows, especially around LMNs.
But compliance rules are very clear:
- The LMN must be completed by the evaluating clinician, not by the supplier, ATP, or another party
- It must be completed by the person performing the specialty wheelchair evaluation, meaning the LMCP with no financial relationship to the equipment supplier
- The LMCP must document the evaluation and other aspects of patient care in a medical record created and maintained by the therapist
- AI is new to CRT, and there are some guidelines released by CMS with more to come
Suppliers can support tools or portals, but they cannot install or control software within the clinician’s system. And even when tools are used, the clinician must still document the evaluation independently.
This reinforces a key point. AI can support efficiency, but it cannot replace ownership.
Telehealth in CRT
Prior to 2020, telehealth was limited:
- It was largely limited to beneficiaries in rural areas
- It had to be performed at an originating site
- Beneficiaries still had to travel for virtual encounters
In March 2020, the public health emergency introduced waivers that removed many in-person requirements. As a result, telehealth expanded significantly during COVID.
Those waivers:
- Enabled virtual care to reduce COVID-19 exposure
- Expanded telehealth across face-to-face exams with treating practitioners
- Allowed wheelchair evaluations with LMCPs such as PTs and OTs
- Allowed ATP assessments, home assessments, and required signatures
- Permitted visits in the beneficiary’s home, removing the originating site requirement
Providers were required to continue meeting coverage criteria while also reducing exposure risk.
Once the public health emergency ended in May 2023, the flexibility of telehealth narrowed again.
Today, many waivers have expired, including:
- ATP assessments
- Home assessments
- Signature requirements
However, some flexibilities were extended through December 31, 2027:
- Treating practitioner visits
- LCMP wheelchair evaluations
An ATP can still perform assessments virtually for beneficiaries who reside in remote or rural areas.
What matters most is this: telehealth does not change coverage requirements. It only changes how certain interactions can occur.
There is also a difference between what is allowed and what is advisable. Telehealth should be used intentionally, not universally.
Expansion of telehealth has brought increased CMS scrutiny to prevent abuse. Overuse or misuse can trigger concerns around abuse or overutilization.
Telehealth should only be used when it supports the best outcome for the specific situation. It should not be treated as all or nothing. Each case is different.
What telehealth looks like in practice
- Start with a virtual screening to determine whether a telehealth wheelchair evaluation is appropriate
- Move to an in-person evaluation if needed, with ATP and LMCP involvement as appropriate
Experience and judgment matter
- Lack of experience can lead to poor outcomes, including ill-fitted equipment, reduced MRADL performance, or equipment that cannot be used in the home due to environmental barriers
- Risk increases if physical or cognitive impairments cannot be clearly observed virtually
- If key areas cannot be properly evaluated, they must be deferred to an in-person visit
When it’s appropriate and when it’s not
Telehealth may be appropriate for:
- Experienced users receiving replacement chairs with no significant changes
- Early-stage neuromuscular conditions such as ALS or MS without complex deformities
- Telehealth is generally not appropriate for:
- New end-users, such as a spinal cord injury patient receiving their first wheelchair
- Advanced or complex conditions
- Cases where physical assessment is critical
Telehealth is generally not appropriate for:
- New end-users, such as a spinal cord injury patient receiving their first wheelchair
- Advanced or complex conditions
- Cases where physical assessment is critical
What’s next for telehealth?
The CONNECT for Health Act of 2025 (HR4206) has 186 co-sponsors and aims to make telehealth flexibilities permanent.
The Senate companion bill (S.1261) has 96 co-sponsors.
If passed or extended, current telehealth flexibilities may continue.
Repairs, Replacement, and the 5 Year Rule
This is one of the most nuanced areas in CRT.
DME follows a 5-year reasonable useful life. This includes new, used purchase, or rented wheelchairs.
The 5-year period begins when the equipment is delivered to the beneficiary on the date of service, not the age of the equipment itself.
Within that period, equipment:
- Can be repaired due to normal wear from everyday use, up to the cost of replacement including parts and labor
- Cannot be replaced due to normal wear
- Can only be replaced due to loss, such as theft, fire, flood, natural disaster, or a one-time accident
Medicare will not pay for repairs or replacement due to abuse or neglect.
For repairs, documentation must include:
- A technician work ticket
- What was done
- Why it was done
- Itemized labor per part
- Proof of continued need
Continued need must be documented within 12 months of the repair date.
Before 5 Years
Replacement refers to an identical or nearly identical item, meaning codes rather than manufacturer or model.
Equipment the beneficiary owns, or equipment that is a capped rental item, may be replaced in cases of loss or irreparable damage.
If the item is a capped rental with no purchase option, it must remain a rental.
It is also important to distinguish between irreparable damage and irreparable wear:
- Irreparable damage means a specific one-time accident or incident occurred, such as fire, flood, theft, or damage from running into a wall with power center mount leg rests. In that case, the equipment can be replaced.
- Irreparable wear means deterioration sustained from day-to-day usage over time where no specific event can be identified. In that case, the equipment cannot be replaced within 5 years.
Labor cannot be billed for replacement.
When items that normally require prior authorization are replaced due to a disaster under a waiver, prior authorization is not required. This applies to federally declared disasters, such as hurricanes.
In those cases, claims must be billed with the CR modifier and include a narrative describing the disaster.
After 5 Years
Replacement with an identical item after the reasonable useful lifetime is more straightforward but still requires the right documentation.
Include the following with the prior authorization request for PMDs:
- Standard Written Order (SWO) for the PMD base
- Detailed Standard Written Order (DSWO)
- Documentation of continued medical need, such as a chart note or medical recor
If Medicare paid for the original item and medical necessity was already established, only a DSWO and documentation of continued need are required for replacement.
For identical replacements:
- New medical necessity is not required
- The same codes, including the base and all accessory code descriptions
A new face-to-face or specialty wheelchair evaluation is not required for an identical replacement.
However, it is still important to verify that the identical codes remain appropriate, which may involve ATP assessment or LCMP wheelchair evaluation as needed.
Manufacturer name, make, and model are not required on the DSWO.
In fact, best practice is to use a general description of the codes rather than a specific manufacturer, make, and model. This preserves flexibility and does not lock the order into one specific product.
Example:
- Any manufacturer, make, and model coded as K0861 may be provided.
K0861 = Power wheelchair, Group 3 standard, multiple power options, sling/solid seat/back, patient weight capacity up to and including 300 lbs.
Only identical items, meaning the same HCPCS codes, are automatically approved in prior authorization without new medical necessity. Any change in condition or code requires new medical necessity.
Example:
- If a skin protection cushion (E2603) was provided on the original power wheelchair, and the beneficiary now qualifies for a skin protection and positioning cushion (E2607), new medical necessity from the ordering practitioner or PT/OT must be submitted with the prior authorization request.
- If the original power wheelchair did not include seat elevation because it was not covered prior to May 2023, and the beneficiary now qualifies for seat elevation, medical necessity must be established through a specialty evaluation by a PT/OT.
Before or after 5 years
When replacement is driven by a change in medical need and different codes are involved, the requirements change.
Include the following documentation with the request:
- A new face-to-face evaluation, for items that require one, when there is a change in condition or code
- LCMP specialty wheelchair evaluation
- If a new power wheelchair base is ordered, a new SWO completed by the ordering practitioner who performed the face-to-face exam
- WOPD/DSWO
- Medical record documentation supporting:
- The need for the item ordered
- The change in condition, if applicable
What This All Means for CRT Providers
Across every section, the same theme shows up.
The challenge is not understanding the rules, but applying them consistently across real workflows.
The providers who succeed in 2026 are the ones who:
- Remove ambiguity from their processes
- Standardize how work gets done
- Ensure documentation aligns exactly with policy
- Understand the technical details
- Build workflows around them
- Execute consistently across teams
That is what reduces denials, captures revenue, and keeps organizations compliant.
CRT is growing. Demand is strong.
But growth alone does not protect performance. Operational discipline does.
What’s Next?
If you have follow-up questions about the content or want to learn more about U.S. Rehab membership, you can visit www.usrehab.com or reach out to Dan directly:
Dan Fedor
dan.fedor@vgm.com
570-499-8459
If you’re interested in seeing how Nymbl can support your team with billing, workflows, and operational visibility, you can schedule time with us at www.nymblsystems.com/demo.